PrEP and Chronic Hepatitis B
The risk of HBV infection is significantly reduced in people who use TD*/FTC for HIV PrEP, with or without HBV vaccination due to these drugs having dual HIV and Hepatitis B activity.[5-7]
All people who test positive for hepatitis B surface antigen (HBsAg) should be evaluated for the need for HBV treatment, in accordance with ASHM’s guide titled “Hepatitis B for Primary Care” (https://www.hepatitisb.org.au). For HIV PrEP prescribers without experience in the evaluation of HBV infection, co-managing the patient with an infectious disease, sexual health, s100 HBV GP, or liver specialist should be considered. However, to improve follow-up, to increase convenience for the patient, and reduce costs for the patient and the health system, the ASHM PrEP Guideline panel recommend that PrEP monitoring and HBV monitoring should be integrated and performed by the same clinician, at the same visits.[8]
Both TD* and FTC are active against both HIV and hepatitis B virus (HBV) infections, but of these two agents, TD* is the only approved agent for treatment of chronic HBV infection in Australia. Although early clinical trials showed that oral TDF by itself is effective as HIV PrEP,[9] most subsequent studies have assessed the effectiveness of co-formulated TD*/FTC as HIV PrEP, and hence TD*/FTC PrEP has the most comprehensive evidence base. Also, two case reports describe patients who acquired HIV infection whilst receiving TD* alone for treatment of hepatitis B infection theirinfection, their tenofovir plasma levels and prescription refills indicating adequate medication adherence.[10] Hence the ASHM PrEP Guideline Panel recommends that people who meet the criteria for treatment of chronic HBV infection and who are at risk of HIV should receive daily co-formulated TD*/FTC.
Despite previous concerns about the potential for HBV reactivation, hepatitis flares and acute liver failure when PrEP is ceased, emerging data suggests that these outcomes are very uncommon [11] hence the PrEP Guidelines Committee endorses the use of TD*/FTC as HIV PrEP in people with chronic HBV infection.
While currently not PBS-listed for this purpose, tenofovir alafenamide (TAF) is also a safe and effective treatment for HBV infection.[12] As such, people with HBV infection who require HIV prevention can also use daily oral co-formulated TAF/FTC for PrEP. Of note TAF/FTC is TGA-approved for use as PrEP. TAF/FTC is not PBS-listed for use as PrEP, but it can be purchased across the counter using a private prescription, or be imported through the TGA’s self-importation scheme.
Cabotegravir (CAB-LA) has no activity against hepatitis B, and people with viral hepatitis were excluded from clinical trials of CAB-LA PrEP, hence CAB-LA PrEP is not recommended for people living with hepatitis B.
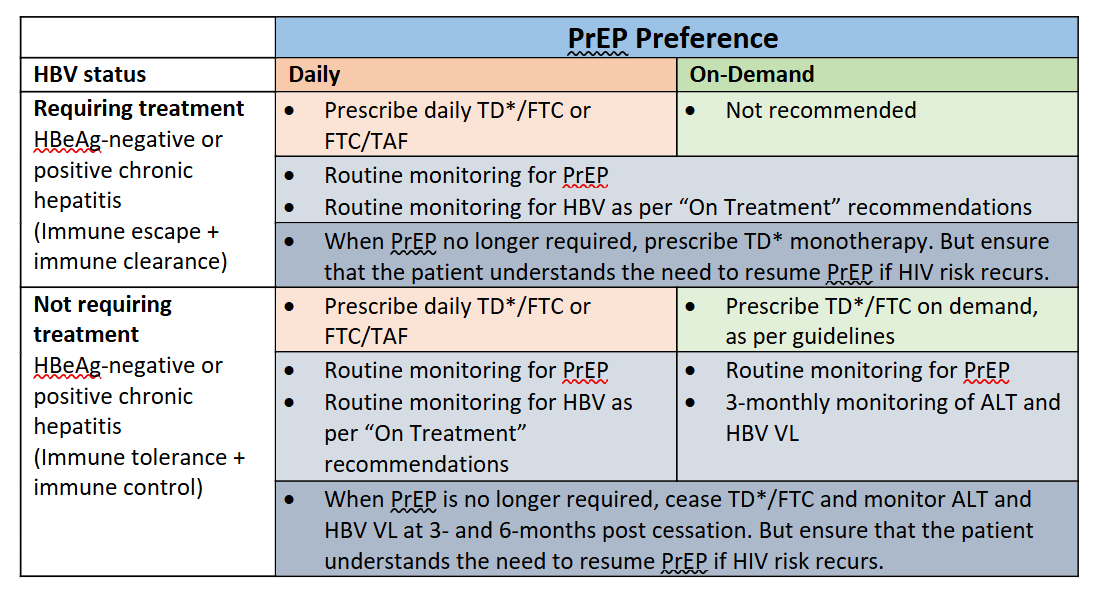
Use of on-demand HIV PrEP in people with chronic hepatitis B infection
Previously, only daily PrEP was recommended for people living with HBV, due to concerns that on-demand PrEP could result in a hepatitis flare on withdrawal of drugs with hepatitis B activity. With further evidence, the WHO now endorses the use of on-demand PrEP using TD*/FTC for people living with HBV under certain circumstances,[2] and the ASHM PrEP Guidelines panel endorses these recommendations, as outlined below.
Circumstances where on-demand TD*/FTC PrEP can be used for people living with chronic HBV infection
- The person does not have cirrhosis of the liver
and/or
- the person does not require treatment of HBV infection, e.g. HBV viral load is < 2000 IU and ALT levels are not elevated
In this setting when the person no longer needs to use on-demand PrEP they can cease TD*/FTC, but they should be monitored at 3 and 6 months after ceasing PrEP for evaluation of HBV reactivation
Circumstances where on-demand TD*/FTC PrEP cannot be used for people living with chronic HBV infection
- the person does have cirrhosis of the liver
and/or
- the person requires treatment of HBV infection e.g. HBV viral load is > 2000 IU and ALT levels are elevated.
If either ALT or HBV VL become elevated during PrEP use or post-PrEP monitoring, advice from an s100 HBV prescriber, sexual health physician, infectious disease physician or gastroenterologist should be sought.
The ASHM PrEP Guidelines panel recommends that PrEP monitoring and HBV monitoring are performed by the same clinician, at the same visits.[8] When PrEP is no longer required, the regimen can be replaced by TD* monotherapy to continue HBV treatment, but the PrEP user needs to understand that future episodes of HIV risk acquisition should be covered by the resumption of TD*/FTC.
REFERENCES
- Molina, J.M., et al., Daily and on-demand HIV pre-exposure prophylaxis with emtricitabine and tenofovir disoproxil (ANRS PREVENIR): a prospective observational cohort study. Lancet HIV, 2022. 9(8): p. e554-e562.
- World Health Organization. Differentiated and simplified pre-exposure prophylaxis for HIV prevention: update to WHO implementation guidance. 2022 Jul 27 [cited 2023 Nov 18]; Available from: https://www.who.int/publications-detail-redirect/9789240053694.
- Shieh, E., et al., Transgender women on oral HIV pre-exposure prophylaxis have significantly lower tenofovir and emtricitabine concentrations when also taking oestrogen when compared to cisgender men. J Int AIDS Soc, 2019. 22(11): p. e25405.
- Hiransuthikul, A., et al., Drug-drug interactions between feminizing hormone therapy and pre-exposure prophylaxis among transgender women: the iFACT study. J Int AIDS Soc, 2019. 22(7): p. e25338.
- Mizushima, D., et al., Effect of tenofovir-based HIV pre-exposure prophylaxis against HBV infection in men who have sex with men. Hepatology, 2023. 77(6): p. 2084-2092.
- Gatanaga, H., et al., Prophylactic effect of antiretroviral therapy on hepatitis B virus infection. Clin Infect Dis, 2013. 56(12): p. 1812-9.
- Heuft, M.M., et al., Protective effect of hepatitis B virus-active antiretroviral therapy against primary hepatitis B virus infection. AIDS, 2014. 28(7): p. 999-1005.
- Schaefer, R., et al., HIV PrEP and viral hepatitis: a unique opportunity for integration. Lancet HIV, 2022. 9(11): p. e745.
- Baeten, J.M., et al., Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med, 2012. 367(5): p. 399-410.
- Fox, J., et al., Tenofovir Disoproxil Fumarate Fails to Prevent HIV Acquisition or the Establishment of a Viral Reservoir: Two Case Reports. Infect Dis Ther, 2016. 5(1): p. 65-71.
- Mohareb, A.M., et al., Risks and benefits of oral HIV pre-exposure prophylaxis for people with chronic hepatitis B. Lancet HIV, 2022. 9(8): p. e585-e594.
- Lubel, J.S., et al., Australian consensus recommendations for the management of hepatitis B. Med J Aust, 2022. 216(9): p. 478-486.